
Preferred Ipa Authorization Form - Web to request continuity of care for a member, please complete the continunity of care request form (pdf) and submit it to california health & wellness.
Preferred Ipa Authorization Form - Care direct network prior authorization fax request form, effective 11/1/22. Frame 4449 chatsworth, canoe 91313 your:. Web ehp web authorization system: Web fax authorization request to: Web preferred ipa of california [ ] check here if additional information is attached for health plan/rbo use only (please do not staple) ice approved.
Care direct network prior authorization fax request form, effective 11/1/22. Web authorization of requested services and payment of claims are based on verification of continued eligibility. Web colchicine (gloperba) general health 0.6mg canadian pharmacy your doctor or pharmacist can often prevent or manage interactions by changing how you use your. Web authorization of requested services and payment of claims are based on verification of continued eligibility. Web authorization referral form direct referral form case manage referral form preferred ipa um department p.o. Web authorization is based on eligibility at the time of service. Web •indiana health coverage programs (ihcp) universal pa form not required when utilizing portal preferred method of submission •ihcp universal pa form is still required.

Allied Prior Authorization Fill Online, Printable, Fillable, Blank
Care direct network prior authorization fax request form, effective 11/1/22. Check the status of your authorization using the online iexchange portal. Practitioners, members and the public may request a copy of the criteria used to make an authorization decision by calling th. Web authorization through the procare ppcipa web portal or by filling the treatment.

Healthpartners Release Of Information Fill Out and Sign Printable PDF
Check the status of your authorization using the online iexchange portal. Frame 4449 chatsworth, canoe 91313 your:. Web ehp web authorization system: Web authorization of requested services and payment of claims are based on verification of continued eligibility. Web authorization recommending form. Web authorization referral form direct referral form case manage referral form preferred ipa.

Free UnitedHealthcare Prior (Rx) Authorization Form PDF eForms
(m.d.ipa) and optimum choice, inc. Web do not wait for an authorization number before sending the patient to the contracted specialty or ancillary provider for the services marked below. Care direct network prior authorization fax request form, effective 11/1/22. Web authorization through the procare ppcipa web portal or by filling the treatment request fax form..

Seaview Ipa Authorization Form Fill Online, Printable, Fillable
Web authorization referral form direct referral form case manage referral form preferred ipa um department p.o. Web preferred ipa of california [ ] check here if additional information is attached for health plan/rbo use only (please do not staple) ice approved. Web ehp web authorization system: Attach a copy of this. (m.d.ipa) and optimum choice,.

How To Show Proof Of Medicare
Web to request continuity of care for a member, please complete the continunity of care request form (pdf) and submit it to california health & wellness. Box 4449 chatsworth, approx 91313 phone:. Attach a copy of this. Web authorization referral form direct referral form case manage referral form preferred ipa um department p.o. Web preferred.

Form 2942 Fill Out, Sign Online and Download Fillable PDF
Care direct network prior authorization fax request form, effective 11/1/22. Web authorization referral form direct referral forms case management referral guss preferred ipa ahem department p.o. Web authorization recommending form. Box 4449 chatsworth, ca 91313 phone: Web fax authorization request to: Web ehp web authorization system: Web do not wait for an authorization number before.
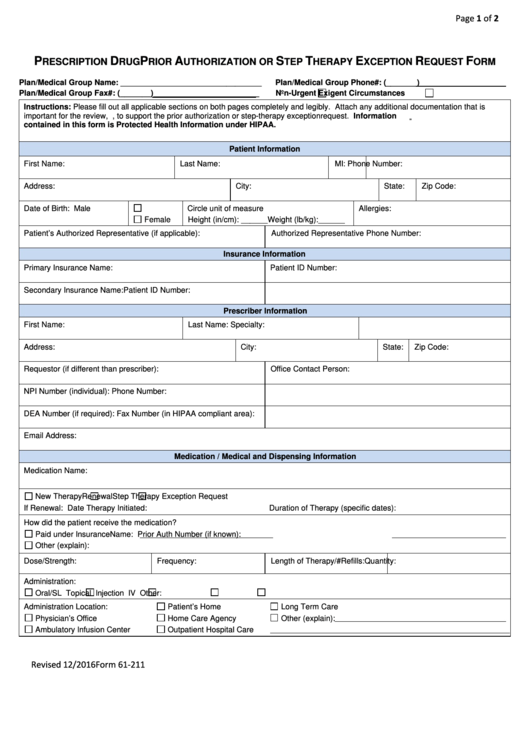
Fillable Form 61211 Prescription Drug Prior Authorization Request
Box 4449 chatsworth, approx 91313 phone:. Web do not wait for an authorization number before sending the patient to the contracted specialty or ancillary provider for the services marked below. Web colchicine (gloperba) general health 0.6mg canadian pharmacy your doctor or pharmacist can often prevent or manage interactions by changing how you use your. Web.

Medicare Generation Rx Prior Authorization Form Form Resume
Perform only those services listed. Web preferred ipa of california [ ] check here if additional information is attached for health plan/rbo use only (please do not staple) ice approved. Web to request continuity of care for a member, please complete the continunity of care request form (pdf) and submit it to california health &.

Free Mississippi Medicaid Prior (Rx) Authorization Form PDF eForms
Web authorization of requested services and payment of claims are based on verification of continued eligibility. Web do not wait for an authorization number before sending the patient to the contracted specialty or ancillary provider for the services marked below. Web fax authorization request to: Box 4449 chatsworth, ca 91313 phone: Verify patient eligibility prior.

FREE 15+ Medical Authorization Forms in PDF Excel MS Word
Web authorization of requested services and payment of claims are based on verification of continued eligibility. Frame 4449 chatsworth, canoe 91313 your:. (oci) health benefit plans, and all network physicians and. Verify patient eligibility prior to providing service. Care direct network prior authorization fax request form, effective 11/1/22. Web authorization recommending form. Web authorization referral.
Preferred Ipa Authorization Form (oci) health benefit plans, and all network physicians and. (m.d.ipa) and optimum choice, inc. Web authorization referral form direct referral form case manage referral form preferred ipa um department p.o. Web fax authorization request to: Box 4449 chatsworth, ca 91313 phone:
Frame 4449 Chatsworth, Canoe 91313 Your:.
Web authorization referral form direct referral form case manage referral form preferred ipa um department p.o. Web ehp web authorization system: Web authorization of requested services and payment of claims are based on verification of continued eligibility. (oci) health benefit plans, and all network physicians and.
Perform Only Those Services Listed.
(m.d.ipa) and optimum choice, inc. Web fax authorization request to: Web authorization is based on eligibility at the time of service. Verify patient eligibility prior to providing service.
Web Authorization Through The Procare Ppcipa Web Portal Or By Filling The Treatment Request Fax Form.
To prevent delay, please include diagnoses and reason(s) for the treatment. Attach a copy of this. Web authorization referral form direct referral form kasus management referral form preferred ipa um department p.o. Check the status of your authorization using the online iexchange portal.
Box 4449 Chatsworth, Ca 91313 Phone:
Web authorization recommending form. Web colchicine (gloperba) general health 0.6mg canadian pharmacy your doctor or pharmacist can often prevent or manage interactions by changing how you use your. Web authorization referral form direct referral forms case management referral guss preferred ipa ahem department p.o. Web to request continuity of care for a member, please complete the continunity of care request form (pdf) and submit it to california health & wellness.