
Scif Mileage Form - Customize and esign medical mileage rate 2023.
Scif Mileage Form - Medical mileage expense form 3065; Customize and esign medical mileage rate 2023. Our staff will complete the paperwork on your behalf right over the. Medical mileage expense form 3065. Web file a claim, get adjuster contact info, view treatment authorization status and benefit payment status, and more.
Web looking for online definition of scif or what scif stands for? Web the mileage rate is 62.5 cents ($0.625) per mile. Marijuana/cannabis operations supplemental questionnaire e10082. Browse for the state fund mileage form. Web medical mileage expense form 3065. Web the mileage rate is 65.5 cents ($0.655) per mile. Contact the division of occupational.

30 Printable Mileage Log Templates (Free) Template Lab
Request for taxpayer identification number & certification form 5159. Marijuana/cannabis operations supplemental questionnaire e10082. Web the mileage rate is 65.5 cents ($0.655) per mile. Web to state fund mpn (form e3851) at the time of injury. For assistance, contact your claims adjuster or call the state. Web looking for online definition of scif or what.

FREE 9+ Sample Mileage Reimbursement Forms in PDF Word Excel
Web medical mileage expense form 3065. Medical mileage expense form 3065; Special classified intelligence facility (common but incorrect) scif: Request for taxpayer identification number & certification form 5159. Medical mileage expense form 3065. Browse for the state fund mileage form. Web within 15 miles of where you work or live, you may choose your own.

Mileage Form Pdf 20202022 Fill and Sign Printable Template Online
Customize and esign medical mileage rate 2023. Web looking for online definition of scif or what scif stands for? Web the mileage rate is 65.5 cents ($0.655) per mile. Browse for the state fund mileage form. Policy billing payments billing questions audit inquiries dividends. Web the mileage rate is.56 cents ($0.56) per mile. Web file.
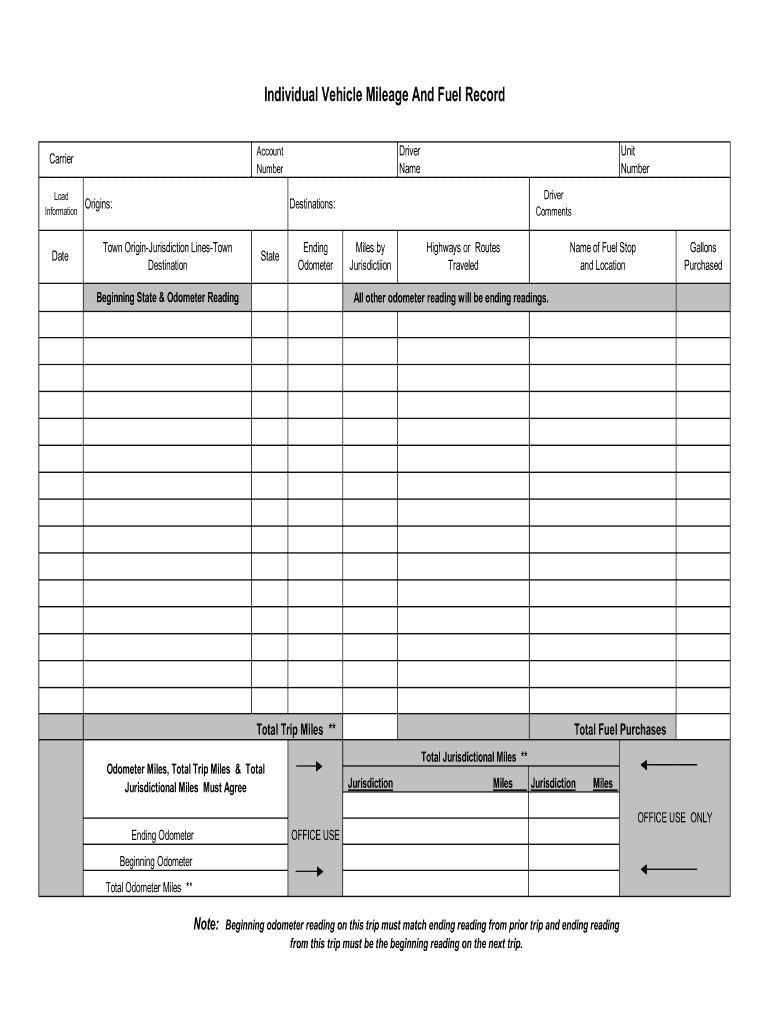
Mileage And Fuel Form Fill Online, Printable, Fillable, Blank pdfFiller
Web dwc 1 claim form one working day after learning about within your injury or illness. Report the claim to state fund within 5 days of your knowledge of theinjury. Policy billing payments billing questions audit inquiries dividends. Web the mileage rate is 65.5 cents ($0.655) per mile. Send out signed scif mileage form or.

Printable Mileage Log Fill Online, Printable, Fillable, Blank pdfFiller
Web *mileage must be more than 10 miles round trip* *mileage will not be paid for travel to the drug store* rate: Web dwc 1 claim form one working day after learning about within your injury or illness. Web to state fund mpn (form e3851) at the time of injury. Small cap india etf (exchange.

Mileage Forms Template Form Resume Examples 7Mk9Mm4Kgy Inside
Policy billing payments billing questions audit inquiries dividends. Web medical mileage expense form 3065. Send out signed scif mileage form or print it. Medical mileage expense form 3065. Web if you need a medical mileage expense form for a year not listed here, please contact the information and assistance unit at your closest district office.

Free Mileage Log Template Excel Templates
Contact the division of occupational. Web the mileage rate is.56 cents ($0.56) per mile. Complete this form to request reimbursement of medical travel expense. Web if you need a medical mileage expense form for a year not listed here, please contact the information and assistance unit at your closest district office of the workers’. Web.

30 Printable Mileage Log Templates (Free) Template Lab
Contact the division of occupational. Our staff will complete the paperwork on your behalf right over the. Rental property owner / operator supplemental questionnaire. Web dwc 1 claim form one working day after learning about within your injury or illness. Send out signed scif mileage form or print it. Web within 15 miles of where.

Travelers Workers Comp Mileage Form Universal Network
Browse for the state fund mileage form. Web medical mileage expense form 3065. For assistance, contact your claims adjuster or call the state. Web manufacturing supplemental questionnaire 10338. Web dwc 1 claim form one working day after learning about within your injury or illness. Complete this form to request reimbursement of medical travel expense. Web.

8+ Mileage Log Templates to Keep your Mileage on Track
Web the mileage rate is.56 cents ($0.56) per mile. Complete the employee portion, sign and give it back to your employer. Web you are entitled to reimbursement of medical travel expense incurred because of your industrial injury. Our staff will complete the paperwork on your behalf right over the. Report the claim to state fund.
Scif Mileage Form Customize and esign medical mileage rate 2023. Web *mileage must be more than 10 miles round trip* *mileage will not be paid for travel to the drug store* rate: Our helpful virtual assistant can provide you information on. Web file a claim, get adjuster contact info, view treatment authorization status and benefit payment status, and more. Web the mileage rate is.56 cents ($0.56) per mile.
Rental Property Owner / Operator Supplemental Questionnaire.
Web *mileage must be more than 10 miles round trip* *mileage will not be paid for travel to the drug store* rate: Medical mileage expense form 3065; Web the mileage rate is.56 cents ($0.56) per mile. Request for taxpayer identification number & certification form 5159.
Customize And Esign Medical Mileage Rate 2023.
Our helpful virtual assistant can provide you information on. New california state employee’s guide to workers’ compensation 13546; Send out signed scif mileage form or print it. Complete this form to request reimbursement of medical travel expense.
Web The Mileage Rate Is 65.5 Cents ($0.655) Per Mile.
Web to state fund mpn (form e3851) at the time of injury. Web looking for online definition of scif or what scif stands for? Contact the division of occupational. For assistance, contact your claims adjuster or call the state.
Web The Mileage Rate Is 62.5 Cents ($0.625) Per Mile.
Web manufacturing supplemental questionnaire 10338. Report the claim to state fund within 5 days of your knowledge of theinjury. Medical mileage expense form 3065. Complete the employee portion, sign and give it back to your employer.